Beyond the Algorithm: Why Brain Worms Expose AI’s Global Diagnostic Blind Spots
- Artificial Intelligence
Arjun Vedanta
- 0
- 5 minutes read
The Human Failure, The Algorithmic Echo
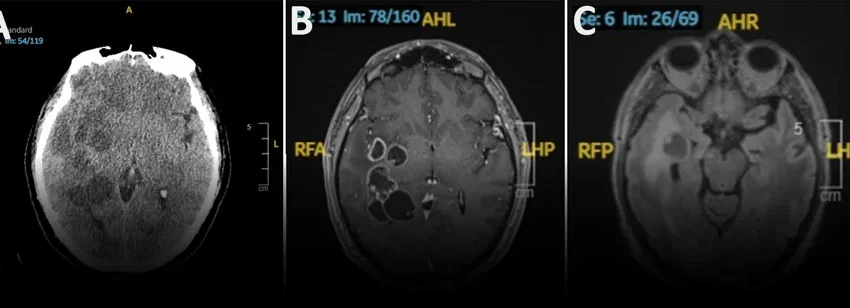
A parasitic infection misidentified as metastatic cancer in a 60-year-old man in Spain offers a stark, chilling lesson for the burgeoning field of diagnostic artificial intelligence. For weeks, the patient experienced persistent headaches and subtle behavioral shifts, prompting doctors to conduct neurological exams and a CT scan. The scan revealed multiple brain lesions and swelling, leading to a strong suspicion of cancer — a plausible diagnosis for a man of that age with such symptoms.
Yet, the initial hypothesis was profoundly wrong. The lesions were not malignant tumors but a rare parasitic infestation. This sequence of events, where human clinicians grappled with an atypical presentation and initially misidentified a critical condition, serves as more than just a medical curiosity. It’s a flashing red light for the often-unquestioned optimism surrounding AI’s role in healthcare diagnostics.
We are told that machine learning algorithms, fed terabytes of medical imaging and patient data, will detect patterns invisible to the human eye, thereby eliminating diagnostic errors. But this Spanish case underscores a critical vulnerability: AI systems are only as good as the data they are trained on, and more importantly, the diversity and representativeness of that data. If human doctors, despite their vast experience, struggled with this edge case, what makes us believe a statistically driven algorithm, likely trained on prevalent conditions from major urban centers, would fare any better?
The push to replace or significantly augment human diagnostic capabilities with AI often overlooks the inherent biases and gaps within existing medical datasets. Rare diseases, unusual presentations, or geographically isolated pathologies simply do not generate enough data points to train robust models. This isn’t a flaw in human reasoning that AI can easily fix; it’s a structural limitation of predictive algorithms operating outside perfectly curated, comprehensive data environments. The narrative that AI always ‘sees’ more clearly than humans collapses when faced with what lies just beyond the statistical mainstream.
The Data Chasm: Local Realities vs. Universal Ambitions
The patient’s history was crucial: he was not immunocompromised and had never traveled internationally. This detail narrowed the epidemiological possibilities for the human doctors, guiding their differential diagnosis away from common tropical parasites. However, for a generalized AI diagnostic system, this specific local context—the prevalence of certain parasites in Spain, or the lack thereof for more exotic ones—is incredibly difficult to integrate effectively without bespoke, hyper-local training data.
Silicon Valley’s approach often tends towards the universal: build one model, scale it everywhere. This ambition crashes hard against the reality of global health. Medical conditions, their manifestations, and their prevalence vary dramatically across different regions, influenced by genetics, environment, diet, and public health infrastructure. An AI model trained predominantly on data from, say, North American or Western European hospitals will inevitably possess significant blind spots when deployed in sub-Saharan Africa or Southeast Asia, where entirely different epidemiological landscapes exist.
The current obsession with ‘universal’ AI models, trained on vast but often geographically skewed datasets, represents a fundamental misunderstanding of biological and epidemiological diversity. It’s a form of digital colonialism, projecting one region’s medical data and priorities onto the rest of the world. For venture-backed AI firms, the incentive is always toward scalability and speed, not necessarily exhaustive accuracy in the most obscure corners of human illness or a painstaking reconciliation of local data nuances.
This case reveals that the critical gaps in diagnostic accuracy aren’t always about processing speed or pattern recognition. They are often about the sparsity of data for uncommon conditions and the profound importance of local, granular epidemiological data that AI models struggle to effectively incorporate. We are consistently underestimating the long tail of human pathologies and overestimating the generalizability of current AI training paradigms.
Rebuilding Trust: Beyond Silicon Valley’s Diagnostic Hubris
The implication for the future of health tech is clear: a truly intelligent diagnostic AI cannot merely be a pattern-matching engine running on a global dataset. It must be adaptable, contextual, and deeply aware of its own limitations. This means investing in decentralized, federated learning approaches where AI models can be trained and fine-tuned on local data, without that data ever leaving its source, ensuring both privacy and relevance. It also demands a greater emphasis on explainable AI, allowing clinicians to understand *why* a system suggested a particular diagnosis, rather than blindly trusting a black box.
International collaboration in building diverse, representative datasets is paramount, but it must be done with robust data governance frameworks that respect data sovereignty and local ethical norms. Instead of a single, monolithic AI, we need a network of specialized, context-aware digital health ecosystems, each attuned to its specific regional challenges. This nuanced approach stands in stark contrast to the prevailing Silicon Valley ethos, which often prioritizes speed-to-market and broad-stroke solutions over the intricate, often messy realities of global human health.
I find it particularly telling that even with advanced medical imaging like CT scans, the human diagnostic journey still involved critical reasoning, eliminating probabilities, and ultimately, a fortunate discovery. AI, in its current form, is a powerful tool for efficiency and scale. But if we allow it to dictate the diagnostic process without built-in mechanisms for humility, local adaptation, and transparency, we risk enshrining a new, technologically driven form of misdiagnosis, overlooking the very human conditions that defy the average statistical curve.